Resuscitation Guidelines
For the latest 2015 Guidelines click HERE and download the specific guideline required
Airway Management
Obstruction of the airway
An unconscious casualty has no control over his or her muscles, including the muscles that control the tongue. The relaxed tongue will fall backwards across the airway, and cause an obstruction. If a breathing unconscious casualty remains on his or her back, the risk of airway obstruction is increased.
An unconscious casualty may also have material in the mouth such as food, blood or vomitus, which may obstruct the airway. It is vital that if such material is present it is removed as soon as possible.
Ensuring an open Airway
Head Tilt/Chin Lift
Head tilt-chin lift manoeuvre is the primary method used to open the airway. To perform the head tilt-chin lift manoeuvre, place one of your hands on the patient’s forehead and apply gentle, firm, backward pressure using the palm of your hand. Place the fingers of the other hand under the bony part of the chin. Lift the chin forward and support the jaw, helping to tilt the head back. This manoeuvre will lift the patient’s tongue away from the back of the throat and provide an adequate airway.
Jaw Thrust
The jaw-thrust manoeuvre is considered an alternate method for opening the airway. This manoeuvre is accomplished by kneeling near the top of the victim’s head, grasping the angles of the patient’s lower jaw, and lifting with both hands, one on each side. This will displace the mandible jawbone) forward while tilting the head backward.
Artificial Airways
Also known as airway adjuncts. 3 types are commonly used by technicians, these are:
- Oro-Pharyngeal
- Naso-Pharyngeal
- Laryngeal Mask Airway
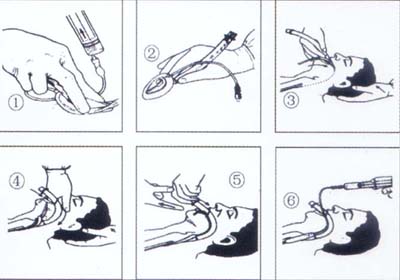
Oro-Pharyngeal (OP)- are used to maintain the airway in the unconscious patient during bag and mask ventilation. They are:
- inserted upside down until the tip is beyond the end of the tongue
- rotated 180 degrees into position
At all times the patient's airway is maintained by the hand not holding the device: holding the mouth open and jaw forward.
An oropharygneal airway is functionally-dependent upon getting the right size; measure from angle of mouth to ear and size the airway against this distance.
Airway Sizes- 00 = Babies
- 0 = Infants
- 1 = Children
- 2 = Small Adults
- 3 = Large Adults
- 4 = V Large Adults
Naso-Pharyngeal (NP) - may be used on conscious victims since it is better tolerated because it generally does not stimulate the gag reflex. Since it is made of flexible material, it is designed to be lubricated and then gently passed up the nostril and down into the pharynx. If the airway meets an obstruction in one nostril, withdraw it and try to pass it up the other nostril.
Laryngeal Mask Airway (LMA) - is used for the purpose of airway management and sits tightly over the top of the larynx it is used as an alternative to Endotraceal Intubation (ET). Although used as an alternative it is believed that it is not as good at securing an airway as the ET route due to the fact it may not protect the airway from aspiration of vomitus. Some ambulance services allow a technician to use this form of adjunct to protect an airway whereas others may not due to the belief that theatre time is required to 'master' it's insertion, although it may be said that the experienced clinician can easily teach the inexperienced how to insert the LMA correctly.
Inserting the LMA:
- Insertion of an LMA (Link to External Site)
Finger Sweep
Probably the simplist means for removing a foreign body can be done by performing a “finger sweep.” This procedure, however, must be performed on unconscious victims only (though not on patient having an epileptic seizure).
Suction - Used for removal of fluids in the mouth e.g. Blood or vomit
Back Slaps, Abdominal Thrusts - See procedure for a choking patient below
Choking Patient - Adult
If blockage of the airway is only partial, the victim will usually be able to clear it by coughing, but if obstruction is complete urgent intervention is required to prevent asphyxia.
Victim is conscious and breathing, despite evidence of obstruction:
- Encourage him to continue coughing but do nothing else
Obstruction is complete or the victim shows signs of exhaustion or becomes cyanosed:
If the victim is conscious:
- Carry out back blows:
-
- Remove any obvious debris or loose teeth from the mouth
- Stand to the side and slightly behind him
- Support his chest with one hand and lean the victim well forwards so that when the obstructing object is dislodged it comes out of the mouth rather than goes further down the airway
- Give
up to 5sharp blows between the scapulae (shoulder blades) with the heel of your other hand; each blow should be aimed at relieving the obstruction, so all 5 need not necessarily be given.
- If the back blows fail, carry out abdominal thrusts:
-
- Stand behind the victim and put both your arms around the upper part of the abdomen
- Make sure the victim is bending well forwards so that when the obstructing object is dislodged it comes out of the mouth rather than goes further down the airway.
- Clench your fist and place it between the umbilicus (navel) and xiphisternum (bottom tip of the sternum). Grasp it with your with your other hand
- Pull sharply inwards and upwards; the obstructing object should be dislodged
- If the obstruction is still not relieved, recheck the mouth for any obstruction that can be reached with a finger, and continue alternating 5 back blows with 5 abdominal thrusts.
If the victim at any time becomes unconscious:
This may result in the relaxation of the muscles around the larynx (voicebox) and allow air to pass down into the lungs. If at any time the choking victim loses consciousness carry out basic life support:Choking Patient - Child
There are a number of different foreign body obstruction sequences each of which has its advocates.
If the child is breathing spontaneously his own efforts to clear the obstruction should be encouraged. Intervention is necessary only if these attempts are clearly ineffective and breathing is inadequate.
- Do not perform blind finger sweeps of the mouth or upper airway as these may further impact a foreign body or cause soft tissue damage
- Use measures intended to create a sharp increase in pressure within the chest cavity, an artificial cough
1. Perform up to FIVE back blows
- Hold the child in a prone position and try to position the head lower than the chest with the airway in an open position
- Deliver up to five smart blows to the middle of the back between the shoulder blades
- If this fails to dislodge the foreign body proceed to chest thrusts.
2. Perform up to FIVE chest thrusts
- Turn the child into a supine position, again with the head lower than the chest and the airway in an open position
- Give up to five chest thrusts to the sternum:
-
- The technique for chest thrusts is similar to that for chest compressions.
- Chest thrusts should be sharper and more vigorous than compressions and carried out at a rate of about 20 per minute.
3. Check mouth
- After five back blows and five chest thrusts check the mouth
- Carefully remove any visible foreign bodies.
4. Open airway
- Reposition the airway by the head tilt and chin lift (jaw thrust) manoeuvre
- Reassess breathing.
5A. If the child is breathing
- Turn the child on his side
- Check for continued breathing
5B. If the child is not breathing:
- Attempt up to 5 rescue breaths to achieve 2 effective
breaths each of which makes the chest rise and fall.
The child may be apnoeic or the airway partially cleared, in either case the rescuer may be able to achieve effective ventilation at this stage - If the airway is still obstructed repeat the sequence as follows:
For a child
- Repeat the cycle (1-5 above) but substitute 5 abdominal thrusts for 5 chest thrusts
-
- Abdominal thrusts are delivered as 5 sharp thrusts directed upwards towards the diaphragm
- Use the upright position if the child is conscious; kneel behind a small child
- Unconscious children should be laid supine and the heel of one hand placed in the middle of the upper abdomen
- Alternate chest thrusts and abdominal thrusts in subsequent cycles
- Repeat the cycles until the airway is cleared or the child breathes spontaneously.
For an infant
- Abdominal thrusts are not recommended in infants because they may rupture the abdominal viscera
- Perform cycles of 5 back blows and 5 chest thrusts only
- Repeat the cycles until the airway is cleared or the infant breathes spontaneously.